Labral Tear
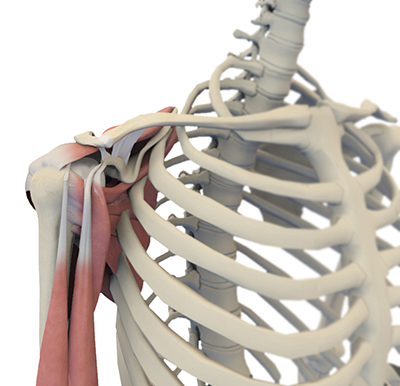
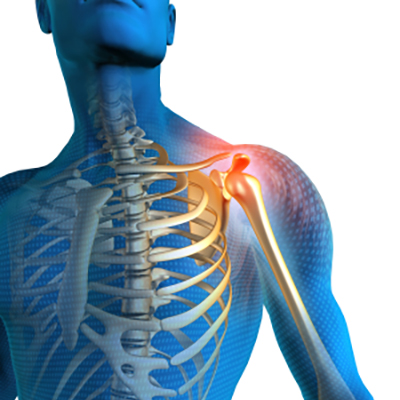
The shoulder joint is a ball and socket joint. A ball at the top of the upper arm bone (the humerus) fits neatly into a socket, called the glenoid, which is part of the shoulder blade (scapula).
The labrum is a ring of fibrous cartilage surrounding the glenoid, which helps in stabilizing the shoulder joint.
The biceps tendon is attached inside the shoulder joint at the superior labrum of the joint. The biceps tendon is a long cord-like structure that attaches the biceps muscle to the shoulder and helps to stabilize the joint.

Labral Tears
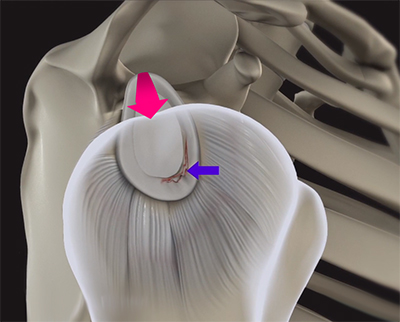
Like other cartilage in the body, the labrum can be subject to injury and tearing. Traumatic injury to the shoulder, such as shoulder dislocations, often result in labral tears. Additionally, overuse of the shoulder by excessive throwing or weightlifting can cause a labral tear. The aging process may also weaken the labrum, leading to injury secondary to wear-and-tear. A shoulder labral tear injury can cause symptoms such as pain, feelings of instability, a catching or locking sensation, and decreased range of motion
The most common types of labral tears include:
- SLAP tear: The term SLAP (superior-labrum anterior-posterior) refers to an injury of the superior labrum of the shoulder at the attachment of the biceps tendon.
- Bankart tear: A Bankart tear is an injury to the labrum that leads to recurrent dislocations and arthritis of the shoulder.
- Posterior labrum tear: Posterior labral tears are often underappreciated and underdiagnosed, but can cause significant pain and functional limitation.
Shoulder Dislocations
The shoulder is one of the most mobile joints in your body. However, because of its mobility, it is also prone to dislocation. This means that the structures of the shoulder might move out of place, causing pain and loss of function in the joint. A dislocated shoulder can be caused by trauma to the upper part of the body, such as a fall, sports injury, or car accident.
Patients with shoulder dislocation commonly exhibit symptoms like:
- Significant pain in upper arm after traumatic injury
- Inflammation, including swelling and bruising.
- Limited function in movement of the arm
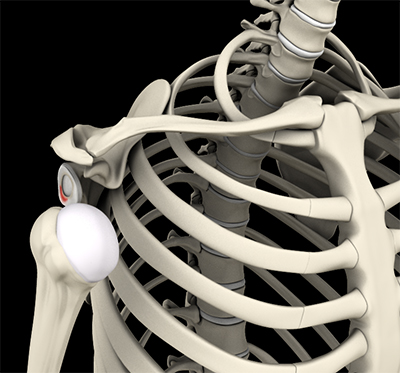
Shoulder Instability
Shoulder instability may occur by injury, overuse, or other genetic factors like joint hypermobility or connective tissue disorders such as Ehlers-Danlos.
The most common form of instability is anterior instability, in which the humeral head predominantly dislocates towards the front of the body. Posterior instability, on the other hand, is experienced when the humeral head predominantly dislocates towards the back of the body. Finally, multidirectional instability is denoted by the dislocation of the humeral head in multiple directions. Given the wide range of factors that may induce shoulder instability, symptoms may include popping, catching, looseness, pain, numbness, or a feeling of “giving way” of the joint.
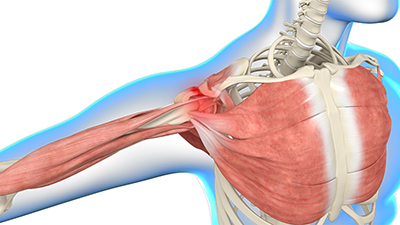
Shoulder Impingement
Shoulder impingement occurs when the bones that make up your shoulder joint compress or rub on the surrounding tissues, causing pain and injury to those tissues.
People who have shoulder impingement may have symptoms like pain while moving their arm up, pain while laying on their side, stiffness, and weakness. This condition can be caused by repetitive motion of the shoulder, such as in sports or activities that require constant overhead motion.
Biceps Tendon Tear
Biceps tendon tears are relatively common injuries that can occur in any of the three tendons of the bicep. Most commonly, tears occur in the two tendons that attach the biceps to the shoulder blade. These tears can be partial thickness or full thickness (tendon is fully detached from the bone). Acute injuries can cause these tears, but they can also arise due to degeneration of the tendon over numerous years.
There are many symptoms that might suggest a biceps tendon tear:
- Sharp pain with lifting or performing overhead movements
- Limited range of motion
- Bruising to upper arm or shoulder
- Weakness in arm or shoulder
- Tenderness and swelling
- Snapping or popping
- “Popeye” deformity (bulge in upper arm)

Diagnosis
Your doctor may suspect a labral tear or other associated injuries to your shoulder based on your symptoms and medical history. Several physical tests will be performed to evaluate the range of motion and stability of your shoulder. X-rays, computed tomography (CT) scan or magnetic resonance imaging (MRI) scan, with a contrast medium, may be ordered to determine the presence of injury. Diagnosis can also be confirmed through a diagnostic shoulder arthroscopy.

Treatment Options
Your doctor may initially suggest conservative approaches such as anti-inflammatory medications and advise rest to relieve symptoms. Rehabilitation exercises may be recommended to strengthen the muscles around your shoulder. If the symptoms are not resolved with these conservative measures, your doctor may recommend shoulder surgery.
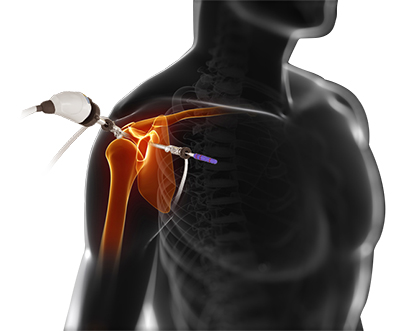
Surgical Options
Shoulder injuries can be treated surgically, oftentimes with a minimally-invasive camera surgery called arthroscopy. Your surgeon makes a few small incisions around the joint. Through one incision, an arthroscope is inserted into the shoulder to visualize the inside of the shoulder joint. Other surgical instruments are inserted through the other incisions to repair the injury or correct anatomy with the help of sutures or anchoring devices. The arthroscope and surgical instruments are then removed, and the incisions are closed.
Resources & References
Fealy, S. (2010). Shoulder Labrum Tears: An Overview. Hospital for Special Surgery.
Johnson CM, DeFoor MT, Griswold BG, Bozzone AE, Galvin JW, Parada SA. Functional Anatomy and Biomechanics of Shoulder Instability. Clin Sports Med. 2024;43(4):547-565. doi:10.1016/j.csm.2024.03.016
A Prospective Analysis of Patients With Anterior Versus Posterior Shoulder ...
Farrar NG, Malal JJG, Fischer J, Waseem M. An Overview of Shoulder Instability and its Management. Open Orthop J. 2013;7:338-346. doi:10.2174/1874325001307010338
Shoulder Instability | University of Michigan Health. Accessed January 20, 2025.